I cannot boast of being a good photographer. Here are a few photos from the past with a bit of explanation. The first photo was taken through an airplane window. The smokiness is real in that without electricity every home has an open fire, and picture was taken early in the morning.
Ethiopia has 70 percent of the mountains found in Africa. The highest is Mount Dashen at 4543m (14930 feet). It also has one of the lowest and hottest places in the world. The Danakil depression is 125m below sea level.The north is also famous for its 11 churches, hewn out of rock. The place is called Lalibela, where an Ethiopian Emperor of that name set out to restore the region to Christianity after a Muslim invasion. The churches are outstanding, being of a single piece of rock! Some believe that English knights, fleeing from Jerusalem during the wars there, helped in the building. This is maybe supported by the inclusion of the English Tudor rose in so many of the carvings. Others say that, at night time, angels came and helped in the building.
There are seven monasteries of the Ethiopian Orthodox Church on Lake Tana from which the Blue Nile starts its journey into Egypt. Above is an example of the multitude of paintings painted in typical Ethiopian style. They are found in abundance in these monasteries. Not in this painting which is of an angel watching over Mary and her Son but interestingly you see amongst the many paintings two saints whom most of the churches don’t recognize. Kidus Pilatus (St Pilate) – sainted because he was the only one who sought to have Jesus released, when he was being tried before His crucifixion. Another called the Cannibal Saint, who supposedly loved eating human flesh but has been sainted because he gave a glass of water to a thirsty girl. The story is that Mary put her hand on the scales when he was being tried after his death.I don’t think they make the horses drink petrol, but these little carts are a very common form of transport in the countryside. Although the car per population ratio is low the car accident per number of cars is very high. One of, if not the highest, in the world.On a straight open bitumen road. Note the rocks placed to warn motorists. It doesn’t help if you are just topping a hill and the rocks start just over the top! See lake Shalla in the distance – the deepest lake in Ethiopia. Its depth is 257 metres and its area 12X15 km.
During our last term in Ethiopia we only had our youngest adopted son living with us. But that meant we had a house full of boys. Three ate with us three or four times a week and there were others from time to time. The memories of those three are precious to us and I might get to write about the other two sometime. I’ll call this one Habtamu, a name which means ‘the rich one’, although he was and is truly poor. As time passed we got to know the history of all of them.
Habtamu was scholastically the brightest of them all. In grade 8 where the pass mark was 37% in the government exam he got 80 something. He was the only one of the three who had a vision of a tertiary education. He was orphaned at age 5. His parents had bought a place in Arba Mintch, and having sold their village place were killed on the way to their new home in a bus crash. Their three children survived. The home which they had bought had 3 rooms. Their eldest child was a girl who was given the responsibility of bringing up her two younger brothers – Habtamu being the youngest. The sister is now married and has a child. Habtamu lives in a little room on the side of the house. He often asked our son to help him in the evenings or weekends when they, like the Israelites in Egypt years before, trod mud and grass together to patch the walls. We paid for all four boys to go to a private school (a cheap one – but they got a full days teaching, whereas in the public schools you only got half day teaching). When we left our son came back to Australia with us. Two of the boys started work but Habtamu wantedto continue his education. Without being lavish we have continued to support him, with the help of a couple of generous people.
He still lives in that same small room on the side of his married sister’s home. But he may well be seen as richer than most because we have bought him a computer and a few other things. Have these things been a blessing? It needsa yes-no answer.
Yes, it has allowed him to continue with his now tertiary education. His score was enough to get him a place in a University but not at the one in his area. He would have to have gone hundreds of kilometres away to do a course which he hadn’t chosen. He still tries to help care for his older brother who studies at a Government University far away. So he elected to go to night school for some extra points and is taking an accountancy course at a private institution. These are courses which have to be paid for.
The answer is ‘no’ because there have been many attempts to break into his room. (The home is not in a good place). A few months ago he was beaten up and ended in the local hospital. His injury was in the upper third of his face and particularly around his right eye with a lot of swelling and some lacerations. Continue reading “Everyone has a story – Habtamu”→
I’m sick of cataloging this afternoon. So here are a few pictures from the past, none medical.
50 + yrs ago. He’s now a grandfather
25 years ago. The school where one of our adopted children attended Solomon – the third teenagerBuilt to safety standards. We eventually got to drive over this bridge! 10 years agoThe house provided for us at one place. My wife went home while I lived around the workers whom I paid to have it fixed. 25 years ago.One of the bed rooms.
Having a family is exciting! Maybe not all beer & skittles but fantastic!
Modern obstetric care in the ‘so called’ first world countries is on the whole excellent. In quoting statistics one must remember the old adage ‘lies, damn lies and statistics’. The internet tells us that in the best countries the maternal mortality rate is 2/100,000 live births. In Ethiopia it is 421/100,000 live births, and I’m sure that it was worse 50 years ago. Around the world there is apparently an obstetric tragedy every 11 seconds. I cannot find figures for maternal deaths when the baby is born dead. That is the world I entered in 1968. This doesn’t include those who live with vesico-vaginal fistulae, of which there are 9,000 new cases annually in Ethiopia (quoted by the late Dr. Catherine Hamlin); nor those who survive ruptured uterus. I’m sure many of these died before they reached a hospital where they could be operated on.
I took out the figures in Soddo (my second long stay in Ethiopia) over a year period and we had a 95% survival rate of those who reached hospital alive. I had reopened the hospital in Soddo in 1993 after the country was freed from the communist era. I was the only surgeon there. I was on call 24/7. After a while we had an obstetrician there who did the day O&G work and was on call at night every second week for obstetric emergencies. But initially I did them all , and later out-of-hours cases every second week. I was also called in to deal with the situation if there was also a ruptured bladder, which occurs in about 10% of cases.
I shall only mention one case here, as I know medicine isn’t everyone’s ‘cup of tea’. My children say they were brought up on such things around the tea table.
In the countryside antenatal care was almost non existent. We ran such a clinic, but few attended and everyone was so busy we didn’t chase things up as hard as we ideally should have done. Most babies were delivered at home. People didn’t come to the hospital until things were obviously seriously wrong. If you lived, for instance, 50km from the hospital, for the majority, there were neither ambulances nor roads so they had to be carried on stretchers over mountainous tracks and crossing waterways. People were frightened to travel at night; and it took, I am told, above 20 people to carry the patient, sharing the work; so it is not surprising that people arrived late.
My first case of ruptured uterus came within a few days of my arriving on my first time in Ethiopia. I was the only doctor in the place. The story apparently was that the labour made no progress, so the native healer tried to do what we call an internal podalic version. In other words by putting his/her hand inside the uterus they intended to turn the baby to get the feet at the bottom so that they could have something to hold onto to attempt to pull the baby out. I don’t know how but whoever it was managed to tear up the front of the vagina and uterus as well as the back of the bladder from top to bottom, and they still could not deliver the baby. The patient obviously rapidly became much sicker and she was brought into the hospital. The baby was dead, but I repaired the long internal tears and she recovered.
The double bubble is what is usually seen in a ruptured uterus
Unfortunately she developed a small fistula for which she was sent to the ‘Hospital by the River’ in Addis. She did well and was later delivered of a healthy child. I’m not sure where she fits into the statistics. Later when I was met with both a bladder as well as a uterine tear I used to bring down some mobilised omentum to separate the uterus and the bladder.
Over my time in Ethiopia I’ve worked in a number of Ethiopian government or University hospitals. I’ve had periods between two and five years over the time that I’ve been there, and for shorter periods in three others. Each morning in all of them it was seen as important to discuss the previous day’s admissions and operations.
A number of medical schools were suddenly started when the government decided they needed more doctors. There are over 20 at the moment, but remember the country’s population is now said to be 105 million. They didn’t have adequate qualified people to teach in any department or even adequate hospital facilities, at least in Arba Mintch.
Just as students began their clinical years of training in Arba Mintch, I transferred from Jimma University to Arba Mintch. I was paid by the University but, added to my University teaching responsibilities, I was expected to be the major surgeon at the hospital.
These, previously described, morning meetings were certainly held for the surgical department in Arba Mintch. I’m not sure about what happened in the other departments. Senior staff, post graduate trainees, interns and students were all meant to attend. In the established universities, where there had been trainees and students for a much longer period there were already buildings appropriate to the needs ; but this was not so in Arba Mintch. In Arba Mintch the University did not have an attached University hospital, so the students were sent to the Government Hospital, which was not given a grant to provide buildings for the students’ needs.
Initially we had 40 students per year, but by the time I left there were 170 per year. There were certain requirements laid down in the University laws which each student had to obey. For instance they had to attend 95% of all lectures and be signed in to have watched 20 operations. Apart from the first year of clinical attachment (4th year) we had students with us all the time as at that time there was no fifth year group. When the numbers were small we had the younger group half the academic year and the other half year we had the more senior class. Although they were with us full time for their attachment we didn’t have them all the time as they had to attend other departments as well. But at the end, because of the increase in numbers, in order to keep groups at a manageable size we had groups from both years all the time time.
This is the group in the adequate room at Jimma.
For our morning meeting the expected attendance was – 3 surgeons; 2 or occasionally 3 post graduate students; 4 interns and up to about 65 students. The shed which we were given had no ceiling, old chairs, without enough for the people and no room for any more. The shed was about 10m by 7m. It is easy to imagine how crowded it was. So, as fortunately most were pretty slim, we could sit two per chair for some of them. I think some of them enjoyed that! We three surgeons had a general hospital to run, as well as the University department to run. In addition we were involved in the teaching programs for nurses, public health workers, anaesthetic students, and a course which tried to teach health assistants basic surgical procedures. Of course there were as well exams to be set and marked. We divided the numbers and apart from the morning meetings, which all had to attend, put a third under the wings of each surgeon. Not, of course, that I’m complaining or that I thought it ridiculous!!
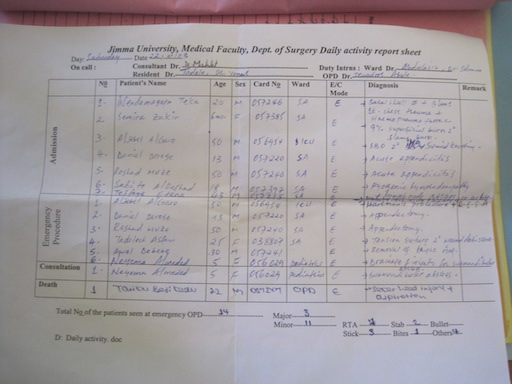
This is about an average number of cases to be presented, assessed, and taught about each morning meeting. Note the doctor’s writing!
The morning meetings lasted about an hour, then one surgeon had a clinical teaching ward round for his third of the students; followed by a ward round for the interns and nurses of the 60 or so patients in the surgical wards. One of the other surgeons was in the operating room. He had his third of the students with him. The third surgeon was in referral clinic with his third of the students.
Dominic Cartier
PS I have opened a second blog under my real name and it deals in a bit more depth and with a few more gory pictures with some of my unusual problems. It is called Medical Memoirs at hicksmedical.wordpress.com