If you feel lonely today – isolated – imagine yourself in one of these crowds or shopping in the street market at the bottom.



Have a great day with your imaginitis!
Dominic Cartier
If you feel lonely today – isolated – imagine yourself in one of these crowds or shopping in the street market at the bottom.
Have a great day with your imaginitis!
Dominic Cartier

I have posted previously about my time working in a leprosarium. Working in a leprosarium 1968-74 And about a non leprosy medical work. The leprosarium extended – part 1 I mentioned there that was more to this other side of the non-leprosy work beyond the medical work.
The Other works for the general community consisted of the following….
A school with an enrolment of about 600 for the surrounding community. This only went to grade 8. A significant number of the pupils were mature age coming to school for the first time to learn the 3Rs. So in grade 1 you might have a six year old sitting next to a 21yo. Teachers were in such short supply that after 3 years as a student you had to become a teacher for a year, before returning to your studies. It seemed to work. One student who went to the leprosy school is now a professor of surgery!
A church with associated outreach. We were in Muslim poorly educated area. So many of our workers in all departments were people from different tribal areas and most were Christians. So the church was several hundred strong. They didn’t have hymn books but many, not being able to read, had developed their ability to memorise. So they had a wide variety of hymns of which they could sing a number of verses. I remember how if a baby would continue crying the preacher would say “haven’t you a breast, woman?”
There was a small administrative unit consisting of the station head and a secretary. They among many other things supervised an electricity generator as often the government service failed. This was a major problem if we were operating at the time the electricity went off line. Operating by torch light while you waited for the generator to be turned on was not fun! But we always kept one handy.
There were mission and government reports to be written, wages to be paid, equipment, medicines etc to be ordered (much of it from overseas, and months in advance). I’m glad someone else had to do it! Continue reading “The extended work – part 2”
I have previously posted about my time working in a leprosarium. Working in a leprosarium 1968-74 I mentioned there the other side of the work carried out on the same station. As leprosy only rarely has acute problems I spent most of my time in the non-leprosy part of the program. I only regularly spent 2 half days/week with the leprosy program, besides seeing the occasional emergency in the leprosy department.
Other work for the general community – this post will only discuss the second non- leprosy medical work. There were several other aspects for another day!
There was an (officially) 30 bed hospital with an added 12 bed TB ward and an attached outpatient clinic.
It was the only hospital covering a large area and several million people. Through the country there were scattered clinics run by dressers (they were not to nurse standard but with some training, and had permission to prescribe a few simple medications) and a few mission clinics but the nearest hospital south was about 80 km away; north 200 km; west 150 km; east several hundred km, and this in a heavily populated, very fertile, part of Ethiopia. We were at the cross roads which led in all 4 directions. At that time cars were few and far between and public transport was limited. As loaded trucks often carried many people on top of their loads we often had mass emergencies if there were major accidents. And there often were!
It really wasn’t beds for just 30 patients. We used to put smaller children one at the head and one at the foot of the bed. In times of great overload we used to sometimes put patients on mattresses under or between the beds. There were verandas on the east and west sides of the main building and we would spread mattresses on them. Sometimes in the rainy season there would be a rush to change the ‘veranda’ patients to the other side away from the rain slanting in from one direction or the other. Most people chose to go to the clinics or to natural healers before a percentage came to us. We could never have survived if all those who should have, had come!
This general hospital had a small ‘operating room’ which was mainly used for obstetrical deliveries which needed forceps deliveries. More major cases, obstetric or other general cases, were taken to the OR in the leprosy hospital. We had few normal deliveries apart from the wealthier women from the nearby moderately large town. For a normal delivery they were charged about ten times as much as a poor person with a complicated pregnancy – something about robbing Peter to pay Paul. Unless there were problems after delivery these ladies were allowed to stay about half an hour.
The room was also used to reduce simple fractures and for suturing. The leaded room with the X-Ray machine was attached to the hospital. The machine was an old WW2 field one. A local young man was trained to take the simpler X-rays. See an example of one of the chest X-rays below.
In addition to the 30 beds there was a 12 bed TB complex. TB was very common. Only the very weak or those with complications, like lung collapse or paralysis from TB of the spine, were admitted. Another national worker was trained to aspirate chests and put in chest drains.
The outpatient department was in a separate building. It included our small pathology department. We treated about 100+ cases a day. Apart from acute emergencies, who were sent directly to the emergency room in the hospital, all were seen initially by a dresser. If they couldn’t make a diagnosis, or if the patient returned with the same problem, they were referred to the nurse. If the problem still remained the nurse arranged for them to see the doctor sometime. I, or if there were 2 one of us, tried to visit outpatients just before I/we went to lunch.
Emergencies were common. I remember one day when 3 ladies with ruptured uterus came within 5 minutes of each other! As well as daytime surgeries, planned or emergency ones, many emergencies arrived out of normal hours, so we operated most nights as well on emergencies.
The 4 nurses had the following duties: One was in charge of the general hospital; one of the leprosy hospital including the OR; one in the leprosy outpatients; one in general outpatients. If we had 5, the fifth was on night duty for all the work – if there were only 4 they rotated around taking responsibility for both parts of the work at night. They were very competent and really acted as junior surgical registrars.
Below the more line is a picture of a chest X-ray of a TB patient. Continue reading “The leprosarium extended – part 1”
I have posted before about our first day in the hospital on our first spell overseas. An introduction to Life in Africa The establishment had a large complex of programs run by a Christian mission. It was on land given by the Emperor’s daughter and it’s distinctive feature was that it was to have a large leprosarium. This was in a period where the concept for many including the government was to keep people suffering from leprosy (Hansen’s disease), certainly those with the infectious variety, apart from the general populous.
The government gave a grant to the mission to help treat 700 patients residing on the land already granted to them. Nearby there was another parcel of land given for the mission to produce food to feed the leprosy patients living on the leprosarium.
The mission took this work very seriously and expanded way beyond just keeping lepers off the streets and treating them in the relatively limited ways available at that time. The work of Drs Cochrane, Brand and Fritschi, basically in India, with their teams had made much progress but treatment was not as available nor efficient as it is today. India was much more developed. I had some time in India with Drs Cochrane and Fritschi on my way to Africa.
The local tribal language was what is now called Oromepha. The greeting was ‘Nega, fiya, urga’ roughly translated ‘hello, how are you? It’s nice to smell you.’ The last bit sounds nasty. But the verb really had broader meaning, including to sense, and I think the intent was something like ‘it’s good to sense your presence’. But because of the use of rancid butter smeared on clothing to make it waterproof, added to smokey fires in houses without chimneys, there was often a fairly powerful smell. When I had been working in the operating room where, in addition to the above, we used a lot of ether for anaesthetics, I personally collected some of the odour. Many times when I got home to greet my wife, with a loving kiss, I got told ‘You stink, go and have a shower.’
Early in our stay, I remember introducing my young son to a lovely bright young man who had come to visit me. The man knew good English. The boy greeted him politely then turned to me and said ‘Dad, do all Ethiopians smell like this?’ The guy was very gracious saying something about kids being like that everywhere!.
The compound had 2 parts. That devoted to leprosy treatment and that for general service to the surrounding community. Today I’ll write about the leprosy part of the work. The general service to the community aspects were almost as extensive! Continue reading “Working in a leprosarium 1968-74”
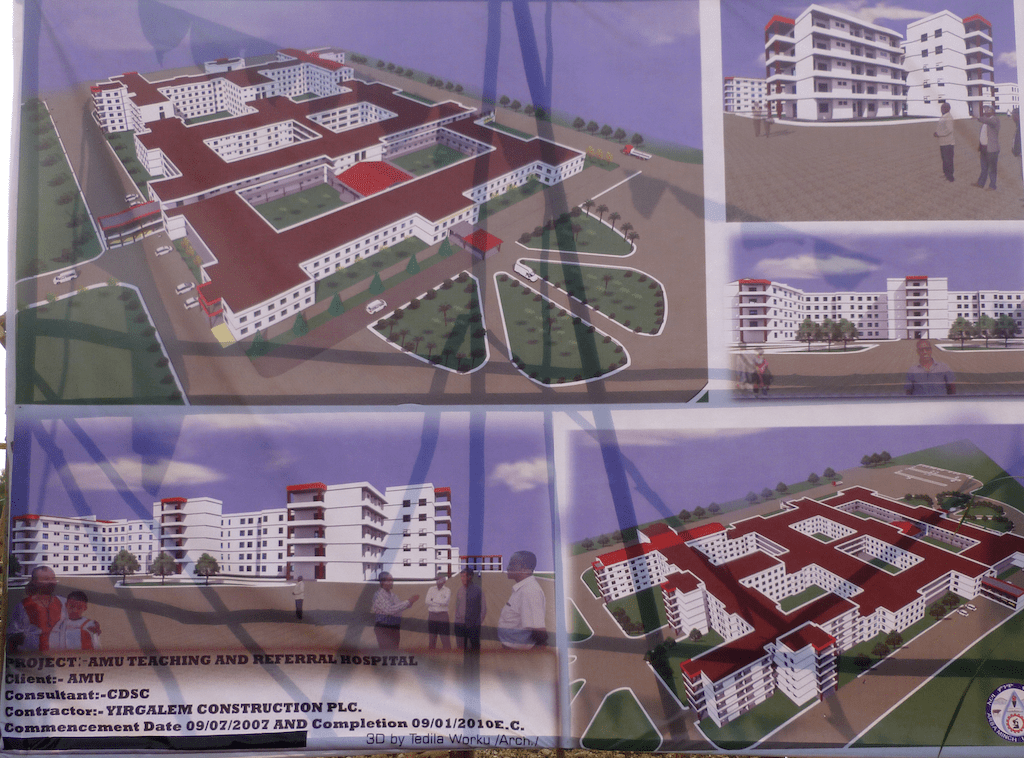
This is a medical post. The above is an elaborate scheme for a designed new hospital to replace the one built initially as a mission hospital by the Norwegian Lutherans. The design had many basic faults. Hopefully they listened and incorporated some changes. It should be opening soon and I trust it will work well. You may note the expected completion date (in our calendar 2017) it was hardly started by then!
You may not want to read beyond the ‘more’ line as there are some very interesting but a bit gory photographs. You can see worse on TV.
I almost always lived and worked in the southern part of the country, between 250 and 500 km from the capital. I had taught briefly in the capital, but that was where the vast majority of the nationals sought to be, so I usually worked down country.
Interestingly I had a postgraduate surgical trainee come down from the capital, as a patient, where he was working in a major teaching hospital for surgery on himself. He brought his own anaesthetist with him. The anaesthetist went to church and prayed while I operated on his colon cancer and my guy gave the anaesthetic. Follow up on Mesfin of the ‘3 Teenagers’
Another man come from the capital of a neighbouring country. He had drunk lye and had a very narrowed scarred oesophagus. He had an oesophagectomy performed and his oesophagus replaced with a piece of colon. We didn’t have a physiotherapist, so essential in the postoperative care of such patients, and I gave a crash course to the servant (slave) he had brought with him. The patient and the servant did well and the patient wrote to me yearly for several years.
But the case I wish to write about today is a man whom I met on arrival as a new professor at a down country University Hospital. He was a poor man with a huge scrotum. When he stood up his scrotum nearly touched the ground. When weighed, after excision, it was 30 kg. There were 2 trained surgeons there but they weren’t prepared to operate on him, even though they were quite senior.
The cause was tuberculosis of his groin lymph glands and if you look at the photo later, you will see that his left leg had begun to swell as well.
The condition is called lymphedema and occurs because the lymph cannot drain back through the diseased nodes which are blocked by the disease. In his case they were affected by TB. Lymph is part of the blood carried out by the arteries which is filtered through the tissues and returned through the lymph channels higher up back into the veins. It has no blood cells in it but is a second return system running parallel in function to the veins. The volume drained as lymph is much less than is returned through the veins. In other words the volume carried out by the arteries equals the volume returned by the veins and the lymph.
Of interest are the following….
So the aim of the surgery is to dissect out the penis and testicles without damaging them; excise the abnormal tissue; cover the defect – creating a new scrotum and covering the penis with skin, often using skin grafts.
Photo 1 shows the patient lying on the operating table prepared for surgery. As he had to be prep’d from the umbilicus down to his feet on the front and back, it was done with him awake and standing up. You will perhaps note the left leg has begun to swell.
Photo 2 shows the penis dissected out before the mass is excised.
Photo 3 shows the dissection complete and awaiting repair.
Photo 4 shows the excised scrotum, which weighed 30 kg.
Several days after surgery I asked him if he had had an erection. With the broadest of smiles – the frustrated young husband said “yes”.
Looking through my photos preparing for this I noted that my first assistant was a postgrad student, who is now working with the Red Cross in South Sudan. He’s a very good young surgeon. After his grandfather died he appointed me as his new g’father replacement.
The photos are below the line. Continue reading “Beware…”
